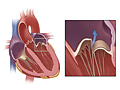
Mitral valve
regurgitation means that one of the valves in your heart-the mitral valve-is
letting blood leak backward into the upper area of the heart.
Heart valves work like
one-way gates, helping blood flow in one direction between heart chambers or in
and out of the heart. The mitral valve is on the left side of your heart. It
lets blood flow from the upper to the lower heart chamber.
When the
mitral valve is damaged-for example, by an infection-it may no longer close
tightly. This lets blood leak backward, or regurgitate, into the upper chamber.
Your heart has to work harder to pump this extra blood.
Small
leaks are usually not a problem. But more severe cases weaken the heart over
time and can lead to
heart failure.
What causes mitral valve regurgitation?
There are
two forms of mitral valve regurgitation: chronic and acute.
Chronic mitral valve regurgitation, the most common type, develops slowly.
Primary regurgitation means there is a problem with the anatomy of the valve. The valve does not work well and does not close tightly. This might happen because of problems like calcium buildup on the valve. It can also happen in people who have mitral valve prolapse.
Secondary regurgitation means another heart problem causes the valve to not close tightly. The anatomy of the valve is typically normal. The heart problem, such as heart failure, affects the heart muscle, and this causes regurgitation.
Acute mitral valve regurgitation develops quickly and can be life-threatening. It
happens when the valve or nearby tissue ruptures suddenly. Instead of a slow
leak, blood builds up quickly in the left side of the heart. Your heart doesn't
have time to adjust to this sudden buildup of blood the way it does with the
slow buildup of blood in chronic regurgitation. Common causes of acute
regurgitation are
heart attack and a heart infection called
endocarditis.
What are the symptoms?
Symptoms of mitral valve regurgitation include being tired or short of breath when you are active.
If your heart weakens because of your
mitral valve, you may start to have symptoms of heart failure. Call your doctor
if you start to have symptoms or if your symptoms change. Symptoms include:
Shortness of breath with activity, which
later develops into shortness of breath at rest and at
night.
Extreme tiredness and weakness.
A buildup of
fluid in the legs and feet, called edema.
Acute mitral valve regurgitation
is an emergency. Symptoms come on rapidly. Symptoms include severe shortness of
breath, fast heart rate, lightheadedness, weakness, confusion, and chest pain.
How is mitral valve regurgitation diagnosed?
Because you may not have symptoms, a specific type of
heart murmur may be the first sign your doctor
notices. Further tests will be needed to check your heart. Tests may
include:
Echocardiograms, which use ultrasound to see how
serious the valve problem is.
Cardiac catheterization to see how serious the problem is.
Finding out that something is wrong with your heart is
scary. You may feel depressed and worried. This is a common reaction. Sometimes
it helps to talk to others who have similar problems. Ask your doctor about
support groups in your area.
How is it treated?
Treatment for chronic cases includes regular tests to check how well the valve and the heart are working. You may take medicines to treat complications. You may take medicine to treat a heart problem that is causing the regurgitation.
You may need to have the mitral valve repaired or replaced. Your doctor will check many things to see if surgery is right for you. These things include the cause of the regurgitation, the anatomy of the valve, if you have symptoms, and how well your heart is pumping blood.
If you have chronic mitral valve
regurgitation, your doctor may want you to make some lifestyle changes to help keep your heart healthy. He or she may advise you to:
Quit smoking and stay away from secondhand
smoke.
Follow a heart-healthy diet and limit sodium.
Be active. Ask your doctor what level and type of exercise is safe for you. You may need to avoid intense activity.
Stay at a healthy
weight, or lose weight if you need to.
Treatment for acute mitral valve regurgitation
occurs while you are in the hospital or the emergency room. You need surgery right away to repair or
replace the valve.
Health Tools
Health Tools help you make wise health decisions or take action to improve your health.
Decision Points focus on key medical care decisions that are important to many health problems.
There are
two forms of mitral valve regurgitation (MR): chronic
and acute. Chronic mitral valve regurgitation develops slowly over several
years. Acute MR develops suddenly.
Chronic mitral valve regurgitation
There are two types of chronic mitral valve regurgitation: primary and secondary.
Primary means there is a problem with the anatomy of the valve. The valve does not work well and does not close tightly.
Primary regurgitation can be caused by:
Calcium buildup as a person ages. The mitral valve may become hard, or calcified,
around the tough ring of tissue (annulus) to which the mitral valve flaps are
attached. Normally the mitral annulus is soft and flexible. But as a person
ages, calcium may build up inside the annulus. This hardened mitral valve
cannot close completely, and blood leaks backward (regurgitates) into the upper
left chamber of the heart (atrium).
Rheumatic fever, which can scar the heart valves. This can prevent them from closing completely.
Previous use of the
weight-loss medicine fen-phen (phentermine and fenfluramine/dexfenfluramine),
which appears to increase the risk of heart valve disease.
Injury to the heart or the chordae tendineae, which are
strong, flexible cords that control the opening and closing of the mitral
valve.
Secondary means another heart problem is causing the valve to not close tightly. The anatomy of the valve is typically normal. The heart problem affects the heart muscle, and this causes regurgitation.
Secondary regurgitation can be caused by heart problems that affect the left ventricle. These problems include:
Acute mitral
valve regurgitation occurs when the mitral valve or one of its supporting
structures ruptures suddenly, creating an immediate overload of blood volume
and pressure in the left side of the heart. Your heart
doesn't have time to adjust to the increased volume and pressure of blood (as it does in chronic MR).
Causes of sudden rupture include:
Injury to the chordae tendineae. Endocarditis may also cause the chordae
tendineae to rupture.
Injury to the chest.
Heart attack,
which may cause the rupture of the muscle (papillary) surrounding the valve.
Primary MR. If you have
mild-to-moderate primary MR, you
may not have symptoms. If you have severe disease, you may have symptoms when you are active. Symptoms include:
Fatigue and weakness.
Shortness of breath.
Secondary MR. If you have secondary MR, you likely have symptoms of the heart problem that has led to the regurgitation. You may have symptoms of heart failure or coronary artery disease.
Acute mitral valve regurgitation
Acute mitral valve regurgitation is an emergency. Symptoms of acute
mitral valve regurgitation appear suddenly. Most people who develop acute MR
are already in the hospital or emergency room because of another heart problem.
Symptoms include severe shortness of
breath, fast heart rate, lightheadedness, weakness, confusion, and chest pain.
Symptoms of acute mitral valve regurgitation including severe shortness of
breath, fast heart rate, lightheadedness, weakness, confusion, and chest pain.
Call a doctor immediately if you have:
Symptoms of
heart failure, such as shortness of breath, fatigue,
and swelling in the legs and feet.
Mitral valve regurgitation (MR) and are having symptoms of infection such as fever
with no other obvious cause. Be alert for signs of infection if you have
recently have had any dental, diagnostic, or surgical procedure.
A decreased ability to exercise at your usual
level.
Excessive fatigue (without other explanation).
If you are coughing up blood, call a doctor immediately.
Watchful waiting
Watchful waiting is a
wait-and-see approach. If you do not have symptoms of MR, your doctor will
still want to see you for regular checkups. Your doctor will want to see you as soon as you have symptoms for
the first time. If your doctor has talked with you about what to do if you have
symptoms, follow your doctor's instructions. Contact your doctor if your
symptoms get worse.
Who to see
Health
professionals who can evaluate symptoms that may be related to mitral valve
regurgitation include:
They frequently can also order the tests needed for
further evaluation of symptoms.
Exams and Tests
Chronic
mitral valve regurgitation (MR) can be difficult to
diagnose. It is a "quiet" condition and often has no symptoms, or your symptoms
may be confused with other heart-related conditions.
Chronic MR is
often diagnosed during a routine checkup or a visit to the doctor for another
condition. A
heart murmur may be the first sign leading your doctor
to the diagnosis, especially if you have no other symptoms.
Acute
MR causes sudden symptoms and is much less common than chronic mitral valve
regurgitation. It is usually diagnosed while you are already hospitalized or in
the emergency room.
When your doctor suspects you have MR, he or
she will discuss your medical history, do a physical exam, and likely
order tests to check your heart. Your doctor uses the information to find out how severe your MR is. For more information, see Mitral Valve Regurgitation: Severity.
Medical history and physical exam
To
find out the severity of your MR, your doctor will ask you to describe the
symptoms you are experiencing, such as shortness of breath, fatigue, or chest
pain.
During the physical exam, the doctor will take your blood
pressure, check your pulse, listen to your heart and lungs, look at the veins
in your neck (jugular veins), and check your legs and feet for fluid buildup
(edema).
Echocardiogram
Echocardiogram (sometimes called an echo or
echocardiography) is a type of
ultrasound exam. It helps your doctor find out how severe your MR is. Also, echocardiography can help
determine whether the heart's main pumping chamber (left ventricle) is
functioning properly, whether any structural problems exist that may affect the
mitral valve, and whether the chambers of the heart are enlarged.
Electrocardiogram
An
electrocardiogram (EKG, ECG) is a test that measures
the electrical signals that control the rhythm of your heartbeat.
Although the EKG may reveal abnormal electrical activity
in the heart, further testing is often still needed to find out the severity
of MR and to confirm whether MR is causing enlargement of the left ventricle.
The result of an EKG is often normal in people who have mild MR.
Imaging tests
A
chest X-ray may be done to evaluate heart size and to
assess symptoms of MR, such as shortness of breath. Calcium deposits on the
heart valves may sometimes be seen on a chest X-ray.
A magnetic resonance imaging (MRI) test may be done to see how well the heart is pumping blood and to check how severe the MR is.
Cardiac catheterization
Cardiac catheterization may be done to confirm the severity of mitral valve leakage
seen on an echocardiogram.
Regular checkups
How often you see your
doctor and what tests are done will be determined by how severe your chronic
mitral valve regurgitation is.
Recommended frequency for checking mitral valve regurgitationfootnote 1
Severity of mitral regurgitation
How often you should have an echocardiogram
Mild
Every 3 to 5 years
Moderate
Every 1 to 2 years
Severe
At least every 6 to 12 months
Treatment Overview
Treatment for chronic mitral valve regurgitation (MR) includes monitoring
your heart function and symptoms. It may include treating symptoms as they develop.
If another heart problem has caused the regurgitation, you will get treatment for that heart problem. If MR becomes severe, the mitral valve may need to be repaired or replaced.
Treatment for acute MR is immediate. Medicines and
urgent surgery are usually needed.
Chronic regurgitation
Treatment depends on whether
you have primary MR or secondary MR. It also depends on if you have symptoms or complications and how severe the regurgitation is.
Monitoring. If you don't have
symptoms and you only have mild-to-moderate regurgitation, your doctor may only
monitor your heart and valve function with an
echocardiogram. You will see your doctor regularly. How often you get this test depends on the severity of regurgitation. For more information, see Exams and Tests.
Medicine. Your doctor may prescribe
medicines to treat complications or treat the heart problem that caused the mitral regurgitation. For more information, see Medications.
Valve replacement or repair. Surgery may be done to replace the mitral valve. Surgery or a procedure may be done to repair the mitral valve. For more information, see Surgery.
Acute regurgitation
Initial treatment for acute MR
includes medicines as needed to stabilize your condition.
If medicines don't help, an
intra-aortic balloon pump may be used for a short time to help circulate blood and ease the workload on your heart. Surgery may be done immediately to replace or repair the valve.
Ongoing Concerns
Chronic
primary mitral valve regurgitation (MR) develops slowly. And
most people go years without having any symptoms. Before symptoms start, your
condition may not be serious and you generally feel good. But even during this
time, MR is doing irreversible damage to your heart. Because of this ongoing
damage, your doctor may suggest a valve repair or replacement before you start having symptoms.
Although it may be difficult to think about a surgery or procedure when you feel well, not
having the valve repaired or replaced could lead to
heart failure.
You will begin to have
symptoms of chronic MR when your heart begins to weaken. A variety of medicines
are available to treat your symptoms as MR progresses and to prevent
complications.
Complications
People with mitral valve
regurgitation sometimes develop serious complications including:
If you smoke, try to quit. Medicines and counseling can help you quit for good. Avoid secondhand smoke too.
Your doctor will also
recommend that you follow a
heart-healthy diet and
limit how much sodium you eat.
Be active, but ask your doctor what level of exercise is safe for you. You may need to be cautious about physical activity if you have
symptoms, irregular heart rhythms, or changes in your heart size or function.
But regular activity, even low-level activity such as walking, will help keep
your heart healthy. If you want to start being more active, talk to your doctor
first. Your doctor will help you create a safe exercise plan. For more information, see Mitral Valve Regurgitation and Exercise.
If you need to lose weight, try to reach and stay at a healthy weight. For help, see the topic Weight Management.
Take care of yourself
See your doctor right away if you have new symptoms or symptoms that get worse. For more information, see When to Call a Doctor.
See your doctor regularly. And get the tests you need, such as echocardiograms, to assess your heart. For more information, see Exams and Tests.
Manage other health problems including high blood pressure, diabetes, and high cholesterol.
Practice good dental hygiene and have regular checkups.
Good dental health is especially important, because bacteria can spread from
infected teeth and gums to the heart valves.
Get a flu vaccine every year. Get a pneumococcal vaccine shot. If you have had one before, ask your doctor if you need another dose.
Talk with your doctor if you have concerns about sex and your heart. Your doctor can help you know if or when it's okay for you to have sex.
Medications
Medicines do not prevent or correct the
damage to the heart caused by
mitral valve regurgitation (MR). For chronic regurgitation, they might be used to treat complications of mitral regurgitation. They might be used to help treat the heart problem that has caused secondary MR. In acute regurgitation, medicine is used as emergency treatment before surgery.
Chronic regurgitation
In
chronic MR, you may take medicine if you have symptoms and a low ejection fraction. You may take medicine to treat heart failure.
Medicine after surgery
Antibiotics. If you have an
artificial valve, you may need to take
antibiotics before you have certain
dental or surgical procedures. The antibiotics help
prevent an infection in your heart called
endocarditis. You will likely take antibiotics
after surgery to repair or replace a valve. If you
have had rheumatic fever, you may take antibiotics to avoid getting it again.
Blood thinners. Blood thinners prevent blood clots after surgery. Blood thinners include antiplatelet medicine, such as aspirin, or anticoagulant medicine. If you have an artificial heart valve, you may need to take this medicine for the rest of your life.
Acute regurgitation
In acute MR, medicines are used in the hospital to
stabilize your condition until you can have surgery to replace or repair the
valve.
Complications
Medicines are used to prevent or treat complications of mitral regurgitation such as atrial fibrillation or heart failure. For more information, see the topics:
With chronicmitral valve regurgitation (MR), a mitral valve repair or replacement might be recommended. Surgery may be done to replace the mitral valve. Surgery or a procedure may be done to repair the mitral valve. Whether surgery is right for you depends on many things including the cause of MR.
With acute MR, urgent surgery to
repair or replace the valve is usually needed. In some cases, surgery to
correct the cause of acute MR may also be needed.
Chronic regurgitation
Primary MR. Valve repair or replacement is the only cure for primary MR, because the abnormal shape of the mitral valve is causing the regurgitation.
Your doctor will check many things to see if surgery is right for you. Your doctor may check to see if:
Your valve can be repaired.
You have symptoms.
You have severe regurgitation.
Your heart has pumping problems (low ejection fraction).
Your left ventricle is larger than normal.
Repair is typically preferred over replacement. The
decision between repairing or replacing the valve depends on the type of damage
you have. For more information, see the topic Mitral Valve Regurgitation: Repair or Replace the Valve.
Secondary MR. Valve repair or replacement cannot cure secondary MR, because another heart problem is causing the mitral valve to not close properly. Treatment of the heart problem, such as heart failure, may be the right treatment for you. Some people might benefit from a repair or replacement of the mitral valve.
Your doctor will check many things to see if surgery is right for you. Your doctor may check to see if:
You have severe symptoms of heart failure.
You have severe regurgitation.
You are having heart surgery for another problem.
Surgical repair
To repair the valve, the
surgeon may:
Reshape the valve by removing excess valve
tissue.
Add support to the valve ring by adding tissue or a
collar-shaped structure around the base of the valve.
Attach the valve
to nearby cordlike heart tissues (chordal transposition).
Surgical replacement
With
replacement, the badly damaged valve is removed and a mechanical (plastic or
metal) or bioprosthetic valve (usually made from pig tissue) is sewn into
place. Before you have valve replacement surgery, you and your doctor will decide on which type of valve is right for you.
A transcatheter procedure is a new way to repair a mitral valve. It does not require open-heart surgery. It is a minimally invasive procedure. A doctor uses catheters in blood vessels to insert a device in the valve. The device helps keep blood from leaking backward. This may relieve symptoms and improve quality of life. This procedure is available in a small number of hospitals. And it is not right for everyone. It might be done for a person who can't have surgery or for a person who has a high risk of serious problems from surgery.footnote 2
Nishimura RA, et al. (2014). 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation, published online March 3, 2014. DOI: 10.1161/CIR.0000000000000031. Accessed May 1, 2014.
A percutaneous device (MitraClip) for mitral regurgitation (2013). Medical Letter on Drugs and Therapeutics, 55(1432): 103.
Other Works Consulted
Adams DH, et al. (2011). Mitral valve regurgitation. In V Fuster et al., eds., Hurst's The Heart, 13th ed., vol. 2, pp. 1721-1737. New York: McGraw-Hill.
Badiwala MV, et al. (2009). Surgical management of ischemic mitral valve regurgitation. Circulation, 120(12): 1287-1293.
Nishimura RA, et al. (2014). 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation, published online March 3, 2014. DOI: 10.1161/CIR.0000000000000031. Accessed May 1, 2014.
Oakley RE, et al. (2008). Choice of prosthetic heart valve in today's practice. Circulation, 117(2): 253-256.
Otto CM, Bonow RO (2012). Valvular heart disease. In RO Bonow et al., eds., Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 9th ed., vol. 2, pp. 1468-1539. Philadelphia: Saunders.
Rodriguez L, Gillinov AM (2007). Mitral valve disease. In EJ Topol, ed., Textbook of Cardiovascular Medicine. Philadelphia: Lippincott Williams and Wilkins.
Whitlock RP, et al. (2012). Antithrombotic and thrombolytic therapy for valvular disease: Antithrombotic therapy and prevention of thrombosis, 9th ed.-American College of Chest Physicians evidence-based clinical practice guidelines. Chest, 141(2, Suppl): e576S-e600S.
Credits
ByHealthwise Staff Primary Medical ReviewerRakesh K. Pai, MD, FACC - Cardiology, Electrophysiology Martin J. Gabica, MD - Family Medicine E. Gregory Thompson, MD - Internal Medicine Adam Husney, MD - Family Medicine Specialist Medical ReviewerMichael P. Pignone, MD, MPH, FACP - Internal Medicine
Nishimura RA, et al. (2014). 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation, published online March 3, 2014. DOI: 10.1161/CIR.0000000000000031. Accessed May 1, 2014.
A percutaneous device (MitraClip) for mitral regurgitation (2013). Medical Letter on Drugs and Therapeutics, 55(1432): 103.
This information does not replace the advice of a doctor. Healthwise, Incorporated, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use. Learn how we develop our content.