



Sigmoidoscopy (Anoscopy, Proctoscopy)
Test Overview
Anoscopy, proctoscopy, and sigmoidoscopy tests allow your doctor to look at the inner lining of your anus, your rectum, and the lower part of the large intestine (colon). These tests are used to look for abnormal growths (such as tumors or polyps), inflammation, bleeding, hemorrhoids, and other conditions (such as diverticulosis).
These tests use different scopes look at different sections of the colon.
- Anoscopy. During an anoscopy, a short, rigid, hollow tube (anoscope) that may contain a light source is used to look at the last 2 in. (5 cm) of the colon (anal canal). Anoscopy can usually be done at any time because it does not require any special preparation (enemas or laxatives) to empty the colon.
-
Proctoscopy. During a proctoscopy, a slightly longer instrument than the anoscope is used to view the inside of the rectum. You will probably have to use an enema or laxative to empty the colon before the test is done.
- The proctoscope is about 10 in. (25 cm) to 12 in. (32 cm) long and 1 in. (2.5 cm) wide. It allows your doctor to look into the rectum and the bottom part of the colon, but it does not reach as far into the colon as the flexible sigmoidoscope.
-
Sigmoidoscopy. During a sigmoidoscopy, a lighted tube is inserted through the anus. Your doctor can remove small growths and collect tissue samples (biopsy) through a sigmoidoscope. You will have to use an enema or laxative (or both) to empty the colon before the test is done.
- The flexible sigmoidoscope is about 2.3 ft (70 cm) long and 0.5 in. (1 cm) wide with a lighted lens system. This instrument allows your doctor to see around bends in the colon.
Flexible sigmoidoscopy is one of many tests that may be used to screen for colon cancer. Which screening test you choose depends on your risk, your preference, and your doctor. Talk to your doctor about what puts you at risk and what test is best for you.
Health Tools
Health Tools help you make wise health decisions or take action to improve your health.
Why It Is Done
These tests are done to:
- Detect problems or diseases of the anus, rectum, or lower large intestine (sigmoid colon). These tests are often done to investigate symptoms such as unexplained bleeding from the rectum, long-lasting diarrhea or constipation, blood or pus in the stool, or lower abdominal pain.
- Remove polyps or hemorrhoids.
- Monitor the growth of polyps or the treatment of inflammatory bowel disease.
- Screen for colon cancer or polyps.
How To Prepare
Anoscopy
Usually, no preparation is needed for an anoscopy.
Proctoscopy and sigmoidoscopy
Test preparation for a proctoscopy and sigmoidoscopy may be similar. Before the test:
- Talk with your doctor to find out if you need to stop taking some medicines, such as aspirin or other blood thinners, before the test.
- Tell your doctor if you have a history of intestinal problems or had surgery recently.
The preparation for these tests usually involves a thorough cleaning of the lower colon, because it must be completely clear of stool (feces). Even a small amount of fecal material can affect the accuracy of the test.
- You may be instructed to follow a liquid diet for 1 to 2 days before the test.
- You may be instructed to not eat for up to 12 hours before the test.
- You may need to have two enemas before the examination.
- You may not need special preparation, especially if you have watery or bloody diarrhea.
Talk to your doctor about any concerns you have regarding the need for this test, its risks, how it will be done, or what the results may mean. To help you understand the importance of this test, fill out the medical test information form (What is a PDF document?).
How It Is Done
You will most likely lie on your left side during the test. You may also be asked to kneel on the table with your bottom raised in the air.
Once you are in position:
- Your doctor will gently insert a gloved finger into your anus. For men, your doctor will also check the condition of the prostate gland.
- The lubricated scope is then inserted. The scope is moved slowly forward into the rectum and lower colon. During a sigmoidoscopy, puffs of air sometimes are blown through the scope to open the colon so that your doctor can see more clearly.
- Suction may be used to remove watery stool, enema liquid, mucus, or blood through the scope.
- Once your doctor has moved the scope forward as far as possible, it is slowly withdrawn while tissue is carefully inspected.
- Your doctor may also insert tiny instruments (forceps, loops, swabs) through the scope to collect tissue samples (biopsy) or to remove growths. Tissue samples may be sent to a laboratory for examination.
The entire examination usually takes 5 to 15 minutes, slightly longer if tissue samples are taken or if polyps are removed.
After the test
After the scope is removed, your anal area will be cleaned with tissues. If you are having cramps, passing gas may help relieve them.
If you received a sedative during the test, do not drive, operate machinery, or sign legal documents for 24 hours after the test. Arrange to have someone drive you home after the test.
After the test you may resume your regular diet, unless your doctor gives you other directions. Be sure to drink plenty of liquids to replace those you have lost during the preparation for the sigmoidoscopy.
How It Feels
An anoscopy, proctoscopy, and sigmoidoscopy examination can be uncomfortable. You may have cramping, a feeling of pressure or bloating, or feel a brief, sharp pain when the scope is moved forward or when air is blown into your colon. As the scope is moved up the colon, you may feel the need to have a bowel movement and pass gas. If you are having pain, tell your doctor.
The removal of tissue samples (biopsy) from the colon does not cause discomfort. A local anesthetic is used when a biopsy of the anal area is done. Your anus may be sore for a few days.
You may have mild gas pains and may need to pass some gas after the procedure. Walking may help relieve the gas pains.
If a biopsy was done or a polyp removed, you may have traces of blood in your stool for a few days.
Risks
There is very little risk of complications from having an anoscopy, proctoscopy, or sigmoidoscopy.
- There is a slight chance of piercing the colon (perforation) or causing severe bleeding by damaging the wall of the colon. But these problems are rare.
- There is also a slight chance of a colon infection (very rare).
Call your doctor immediately if you have:
- Heavy rectal bleeding.
- Severe abdominal pain.
- A fever.
Results
Anoscopy, proctoscopy, and sigmoidoscopy tests allow your doctor to look at the inner lining of your anus and rectum and the lower part of the large intestine (colon).
Your doctor should be able to discuss some of the findings with you immediately after the test. Lab results (such as from a biopsy) may take several days.
|
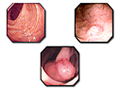
Normal: |
|
|
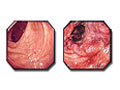
Abnormal: |
Abnormal findings include:
|
Your doctor will discuss any significant abnormal results with you in relation to your symptoms and past health.
What Affects the Test
Reasons you may not be able to have the test or why the results may not be helpful include:
- Stool in the colon or rectum.
- The structure of the colon, such as a colon that has many turns.
- A barium enema done within a week before sigmoidoscopy.
- You have peritonitis, diverticulitis, toxic megacolon, or you have had recent bowel surgery.
What To Think About
- Follow-up tests, such as colonoscopy, may be needed after sigmoidoscopy. A colonoscopy may also be needed to examine the upper section of the colon if growths were seen during sigmoidoscopy. To learn more, see the topic Colonoscopy.
- In some cases, the sigmoidoscope may be attached to a video monitor and a recording device that lets your doctor see the inside of the colon and record the findings.
- Experts recommend routine colon cancer testing for everyone age 50 and older who has normal risk for colon cancer. Your doctor may recommend earlier or more frequent testing if you have a higher risk for colon cancer. Talk to your doctor about when you should be tested.
- Which screening test you choose depends on your risk, your preference, and your doctor. Talk to your doctor about what puts you at risk and what test is best for you.
Related Information
References
Other Works Consulted
- Chernecky CC, Berger BJ (2013). Laboratory Tests and Diagnostic Procedures, 6th ed. St. Louis: Saunders.
- Fischbach FT, Dunning MB III, eds. (2009). Manual of Laboratory and Diagnostic Tests, 8th ed. Philadelphia: Lippincott Williams and Wilkins.
- Pagana KD, Pagana TJ (2010). Mosby's Manual of Diagnostic and Laboratory Tests, 4th ed. St. Louis: Mosby Elsevier.
Credits
ByHealthwise Staff
Primary Medical Reviewer Adam Husney, MD - Family Medicine
E. Gregory Thompson, MD - Internal Medicine
Kathleen Romito, MD - Family Medicine
Arvydas D. Vanagunas, MD, FACP, FACG - Gastroenterology
Current as ofMarch 28, 2018
- Top of Page
Next Section:
Health Tools
Previous Section:
Test Overview- Top of Page
Next Section:
Why It Is Done
Previous Section:
Health Tools- Top of Page
Next Section:
How To Prepare
Previous Section:
Why It Is Done- Top of Page
Next Section:
How It Is Done
Previous Section:
How To Prepare- Top of Page
Next Section:
How It Feels
Previous Section:
How It Is Done- Top of Page
Next Section:
Risks
Previous Section:
How It Feels- Top of Page
Next Section:
Results
Previous Section:
Risks- Top of Page
Next Section:
What Affects the Test
Previous Section:
Results- Top of Page
Next Section:
What To Think About
Previous Section:
What Affects the Test- Top of Page
Next Section:
Related Information
Previous Section:
What To Think About- Top of Page
Next Section:
References
Previous Section:
Related Information- Top of Page
Next Section:
Credits
Previous Section:
References- Top of Page
Current as of: March 28, 2018