Urinary incontinence is the accidental release of urine. It can happen when you cough, laugh, sneeze, or jog. Or you may have a sudden need to go to the bathroom but can't get there in time. Bladder control problems are very common, especially among older adults. They usually don't cause major health problems, but they can be embarrassing.
Incontinence can be a short-term problem caused by a urinary tract infection, a medicine, or constipation. It gets better when you treat the problem that is causing it. But this topic focuses on ongoing urinary incontinence.
There are two main kinds of urinary incontinence. Some women-especially older women-have both.
Stress incontinence occurs when you sneeze, cough, laugh, jog, or do other things that put pressure on your bladder. It is the most common type of bladder control problem in women.
Urge incontinence happens when you have a strong need to urinate but can't reach the toilet in time. This can happen even when your bladder is holding only a small amount of urine. Some women may have no warning before they accidentally leak urine. Other women may leak urine when they drink water or when they hear or touch running water. Overactive bladder is a kind of urge incontinence. But not everyone with overactive bladder leaks urine.
Problems or damage either in the urinary tract or in the nerves that control urination.
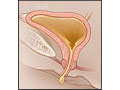
Stress incontinence can be caused by childbirth, weight gain, or other conditions that stretch the pelvic floor muscles. When these muscles can't support your bladder properly, the bladder drops down and pushes against the vagina. You can't tighten the muscles that close off the urethra. So urine may leak because of the extra pressure on the bladder when you cough, sneeze, laugh, exercise, or do other activities.
Urge incontinence is caused by an overactive bladder muscle that pushes urine out of the bladder. It may be caused by irritation of the bladder, emotional stress, or brain conditions such as Parkinson's disease or stroke. Many times doctors don't know what causes it.
What are the symptoms?
The main symptom is the accidental release of urine.
If you have stress incontinence, you may leak a small to medium amount of urine when you cough, sneeze, laugh, exercise, or do similar things.
If you have urge incontinence, you may feel a sudden urge to urinate and the need to urinate often. With this type of bladder control problem, you may leak a larger amount of urine that can soak your clothes or run down your legs.
If you have mixed incontinence, you may have symptoms of both problems.
How is urinary incontinence diagnosed?
Your doctor will ask about what and how much you drink. He or she will also ask how often and how much you urinate and leak. It may help to keep track of these things using a bladder diary for 3 or 4 days before you see your doctor.
Your doctor will examine you and may do some simple tests to look for the cause of your bladder control problem. If your doctor thinks it may be caused by more than one problem, you will likely have more tests.
How is it treated?
Treatments are different for each person. They depend on the type of incontinence you have and how much it affects your life. After your doctor knows what has caused the incontinence, your treatment may include exercises, bladder training, medicines, a pessary, or a combination of these. Some women may need surgery.
There are also some things you can do at home. In many cases, these lifestyle changes can be enough to control incontinence.
Cut back on caffeine drinks, such as coffee and tea. Also cut back on fizzy drinks like soda pop. And don't drink more than one alcohol drink a day.
Eat foods high in fiber to help avoid constipation.
Don't smoke. If you need help quitting, talk to your doctor about stop-smoking programs and medicines. These can increase your chances of quitting for good.
Go to the bathroom at several set times each day, and wear clothes that you can remove easily. Make your path to the bathroom as clear and quick as you can.
Keep track of your symptoms and any leaking of urine with a bladder diary. This can help you and your doctor find the best treatment for you.
If you have symptoms of urinary incontinence, don't be embarrassed to tell your doctor. Most people can be helped or cured.
How can you prevent urinary incontinence?
Strengthening your pelvic muscles with Kegel exercises may lower your risk for incontinence.
If you smoke, try to quit. Quitting may make you cough less, which may help with incontinence.
Health Tools
Health Tools help you make wise health decisions or take action to improve your health.
Decision Points focus on key medical care decisions that are important to many health problems.
When these muscles can't support your bladder well, the bladder drops down and pushes against the vagina. Then you can't tighten the muscles that usually close off the urethra. So urine may leak because of the extra pressure on the bladder when you cough, sneeze, laugh, exercise, or do other activities.
This is the most common type of urinary incontinence in women.
A chronic cough from smoking can make stress incontinence worse.
Urge incontinence
Urge incontinence is caused when the bladder muscle involuntarily contracts and pushes urine out of the bladder. Many times doctors don't know what causes this. But sometimes the cause is:
Irritation of the bladder.
Emotional stress.
Brain conditions such as Parkinson's disease or stroke.
Overactive bladder is a kind of urge incontinence. But not everyone with overactive bladder leaks urine. For more information, see the topic Overactive Bladder.
Other types of incontinence
Less common types of urinary incontinence have other causes. These types include:
The main symptom of urinary incontinence is a problem controlling urination.
Symptoms of stress incontinence:
Involuntary release of urine, especially when you cough, sneeze, or laugh
Leaking a small to moderate amount of urine
Symptoms of urge incontinence:
Frequent and sudden uncontrollable need to urinate
May leak a moderate to large amount of urine, although a small amount is possible
It is common for a woman to have symptoms of both types of incontinence. This is called mixed incontinence.
What Happens
Urinary incontinence usually starts gradually and slowly becomes worse. As it gets worse, a woman may:
Avoid going out in public because of embarrassment.
Become less active.
Have physical problems caused by frequent urine contact. These problems may include irritation of the groin area and more frequent urinary tract infections.
Treating the cause of incontinence often gets rid of or controls these problems.
Some bladder problems are temporary. For example, you may have a urinary tract infection that causes incontinence, but the problem goes away after the infection is cured.
What Increases Your Risk
Sometimes several things combine to cause urinary incontinence. For example, a woman may have had multiple childbirths, be older, and have a severe cough because of chronic bronchitis or smoking. All of these might contribute to her incontinence problem.
Physical conditions that make urinary incontinence more likely include:
Medicines and foods that may make urinary incontinence worse include:
Caffeinated and carbonated drinks, such as coffee, tea, and soda pop.
Alcohol drinks.
Prescription medicines that increase urine production (such as diuretics) or relax the bladder (such as anticholinergics and antidepressants).
Smoking.
When To Call a Doctor
Call your doctor if:
You have urinary incontinence that begins suddenly. This is called acute incontinence. It is often caused by urinary tract problems or medicines and can be easily corrected.
The involuntary release of urine is enough of a problem that you need to wear an absorbent pad, or if incontinence interferes with your life in any way.
Don't be embarrassed to discuss urinary incontinence with your doctor. Urinary incontinence is not an inevitable result of aging. Most women with incontinence can be helped or cured.
Watchful waiting
If you have urinary incontinence that develops slowly, you may be able to control the problem yourself. If home treatment is not effective, or if incontinence interferes with your lifestyle, ask your doctor about other treatments.
Who to see
Health professionals who can diagnose and treat urinary incontinence include:
Your health professional may want you to see a urogynecologist.
If you need surgery, it is important to find a surgeon who is experienced in the types of surgical procedures used to treat incontinence.
Exams and Tests
To diagnose the cause of your urinary incontinence, your doctor will ask about your medical history and do a physical exam. It may be easier for you to answer questions if you keep a bladder diary(What is a PDF document?) for 3 or 4 days before you see your doctor.
To check for stress incontinence, your doctor may ask you to cough while you are standing.
Pad test, which can help show how much urine is leaking. You are given an absorbent pad that has been weighed. You wear the pad until urine leaks, and then you return the pad to be weighed again. The increased weight of the pad gives an estimate of how much urine leaked.
Urodynamic testing is expensive. It is typically done only if surgery is being considered or if treatment has not worked for you and you need to know more about the cause. It provides a more advanced way to check bladder function.
The actual tests done in urodynamic testing often vary. They may include:
Cystometry, a series of tests to measure bladder pressure at different levels of fullness.
Postvoid residual (PVR) measurements, which measure the amount of urine that stays in your bladder after you urinate.
X-rays or ultrasound. These are used to examine changes in the position of the bladder and urethra during urination, coughing, or straining.
If the cause of incontinence is not identified by the above tests, more extensive tests may be needed.
Treatment Overview
Urinary incontinence isn't an inevitable result of aging. Most women who have it can be helped or cured.
The best treatment depends on the cause of your incontinence and your personal preferences. Treatments include:
Behavioral training, such as bladder training and timed urination. For more information, see Other Treatment.
Lifestyle changes and pelvic floor (Kegel) exercises. For more information, see Home Treatment.
Behavioral training, exercises and lifestyle changes, and medicines are usually tried first. If the problem does not get better, your doctor may try another treatment or do more tests.
When there is more than one cause for incontinence, the most significant cause is treated first, followed by treatment for the secondary cause, if needed.
Prevention
You may reduce your chances for urinary incontinence by:
Staying at a healthy weight. For more information, see the topic Weight Management.
Quitting smoking. Smoking causes coughing, which can make it harder to control your urine. Quitting smoking relieves coughing. For more information, see the topic Quitting Smoking.
Home Treatment
If you have urinary incontinence, you can take some steps on your own that may stop or reduce the problem.
Set a schedule of urinating every 2 to 4 hours, regardless of whether you feel the need.
Talk with your doctor about all prescription and nonprescription medicines you take. Find out if any of them may be making your incontinence worse.
Use a bladder diary(What is a PDF document?) to keep track of your symptoms and any leaking of urine. Your diary can help you and your doctor find the best treatment for you.
If you have trouble reaching the bathroom before you urinate, try making a clearer, quicker path to the bathroom and wearing clothes that are easily removed (such as those with elastic waistbands or Velcro closures). Or keep a bedpan close to your bed or chair.
Wear a tampon while doing activities such as jogging or dancing to put a little pressure on your urethra and to temporarily slow or stop leakage. Or you may want to try to prevent leaks with a product like Poise Impressa, which you insert like a tampon.
Exercises
Pelvic floor (Kegel) exercises can help women who have any type of urinary incontinence.footnote 1 These exercises are especially useful for stress incontinence. But they may also help urge incontinence.
Lifestyle changes
Losing weight often helps stress incontinence. Remember that effective weight-loss programs depend on a combination of diet and exercise.
Sometimes making lifestyle changes can help with urge incontinence. Try to identify any foods that might irritate your bladder-including citrus fruits, chocolate, tomatoes, vinegars, dairy products, aspartame, and spicy foods-and cut back on them. Also, avoid alcohol and caffeine.
If you smoke, try to quit. This may reduce coughing, which may reduce your problem with incontinence. For more information, see the topic Quitting Smoking.
Take steps to avoid constipation:
Include fruits, vegetables, beans, and whole grains in your diet each day. These foods are high in fiber.
Drink plenty of fluids, enough so that your urine is light yellow or clear like water.
Get some exercise every day. Try to do moderate activity at least 2½ hours a week. Or try to do vigorous activity at least 1¼ hours a week. It's fine to be active in blocks of 10 minutes or more throughout your day and week.
Take a fiber supplement, such as Citrucel or Metamucil, every day if needed. Read and follow all instructions on the label.
Schedule time each day for a bowel movement. Having a daily routine may help. Take your time and don't strain when having a bowel movement.
Medications
Urinary incontinence may be treated with medicines. But in many cases, treatment with behavioral methods (bladder training, timed urination) and Kegel exercises are tried before medicines. These treatments, when combined with medicine, may help some women more than either treatment alone.
Botox is given as a shot to help relax the bladder muscles. You may need to get a shot every 3 months. Side effects may include having pain when you urinate, not being able to urinate easily, and getting a urinary tract infection (UTI). If you get a Botox shot, you may need to take antibiotics to reduce your risk for getting a UTI.
Surgery
There are several different kinds of surgeries to correct stress incontinence, which occurs when weakened pelvic floor muscles allow the bladder neck and urethra to drop. These surgeries seek to lift the urethra, the bladder, or both into the normal position. This makes sneezing, coughing, and laughing less likely to make urine leak from the bladder.
Surgery works to cure stress incontinence better than any other treatment. If other treatments (like pelvic floor muscle exercises) haven't worked to control your incontinence, surgery may be your best option. What kind of surgery you have depends on your preference, your health, and your doctor's experience.
Mixed incontinence means you have both stress incontinence and urge incontinence. Surgery may help women who have mixed incontinence. If surgery works to reduce the stress symptoms, often the urge symptoms cause less bother.
Other types of treatment for urinary incontinence include:
Behavioral methods. These are often the first thing to try. They often work well. They include:
Bladder training (also called bladder retraining). This is used to treat urge incontinence. With bladder training, you slowly increase how long you can wait before having to urinate by trying to delay urination after you get the urge to go.
Biofeedback. This is a technique for learning to control a body function that is not normally under conscious control. It is usually used to teach pelvic floor muscle exercises.
Pelvic floor muscle exercises (Kegels). Kegel exercises can help strengthen some of the muscles that control the flow of urine. These exercises are used to treat urge or stress incontinence.
Acupuncture. There isn't a lot of evidence for how well acupuncture works for urinary incontinence. In one study, comparing bladder-specific acupuncture to sham acupuncture, both groups had less incontinence. But the group with bladder-specific acupuncture didn't have as many episodes of urgency.footnote 2
Before trying behavioral methods or exercise for urinary incontinence, ask your doctor the following questions:
Is behavioral or exercise therapy alone likely to restore bladder control? Mild to moderate cases of common types of incontinence can be cured or greatly improved by these methods.
How long should I try behavioral or exercise techniques before I consider surgery or other treatment methods? Techniques like Kegel exercises don't limit future treatment options (and they may even improve the odds of success for other treatments). So it is best to set a length of time after which the improvement can be evaluated.
Can I use exercises or behavioral methods along with medicine if medicine treatment is recommended? It may be possible to take medicine for a shorter time or to reduce the amount of medicines used if other methods of treatment are combined with medicine.
Dumoulin C, Hay-Smith J (2010). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews (1).
Emmons SL, Otto L (2005). Acupuncture for overactive bladder. Obstetrics and Gynecology, 106(1): 138-143.
Other Works Consulted
Barber MD, et al. (2008). Transobturator tape compared with tension-free vaginal tape for the treatment of stress urinary incontinence. Obstetrics and Gynecology, 111(3): 611-621.
Garley AD, Noor N (2014). Diagnosis and surgical treatment of stress urinary incontinence. Obstetrics and Gynecology, 124(5): 1011-1027. DOI: 10.1097/AOG.0000000000000514. Accessed August 17, 2015.
Hartmann KE, et al. (2009). Treatment of Overactive Bladder in Women. Evidence Report/Technology Assessment No. 187 (AHRQ Publication No. 09-E017). Available online: http://www.ahrq.gov/clinic/tp/bladdertp.htm.
Kirchin V, et al. (2012). Urethral injection therapy for urinary incontinence in women. Cochrane Database of Systematic Reviews (2).
Naumann M, et al. (2008). Assessment: Botulinum neurotoxin in the treatment of autonomic disorders and pain (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology, 70(19): 1707-1714.
Shamliyan TA, et al. (2008). Systematic review: Randomized, controlled trials of nonsurgical treatments for urinary incontinence in women. Annals of Internal Medicine, 148(6): 1-15.
Sung VW, et al. (2007). Comparison of retropubic vs transobturator approach to midurethral slings: A systematic review. American Journal of Obstetrics and Gynecology, 197(1): 3-11.
Tanagho EA, et al. (2008). Urinary incontinence. In EA Tanagho, JW McAninch, eds., Smith's General Urology, 17th ed., pp. 473-489. New York: McGraw-Hill Medical.
Waetjen LE, et al. (2008). Factors associated with worsening and improving urinary incontinence across the menopausal transition. Obstetrics and Gynecology, 111(3): 667-677.
Credits
ByHealthwise Staff Primary Medical ReviewerE. Gregory Thompson, MD - Internal Medicine Adam Husney, MD - Family Medicine Kathleen Romito, MD - Family Medicine Avery L. Seifert, MD, FACS - Urology
Dumoulin C, Hay-Smith J (2010). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews (1).
Emmons SL, Otto L (2005). Acupuncture for overactive bladder. Obstetrics and Gynecology, 106(1): 138-143.
This information does not replace the advice of a doctor. Healthwise, Incorporated, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use. Learn how we develop our content.